MD 1A-1 2002-2026 free printable template
Show details
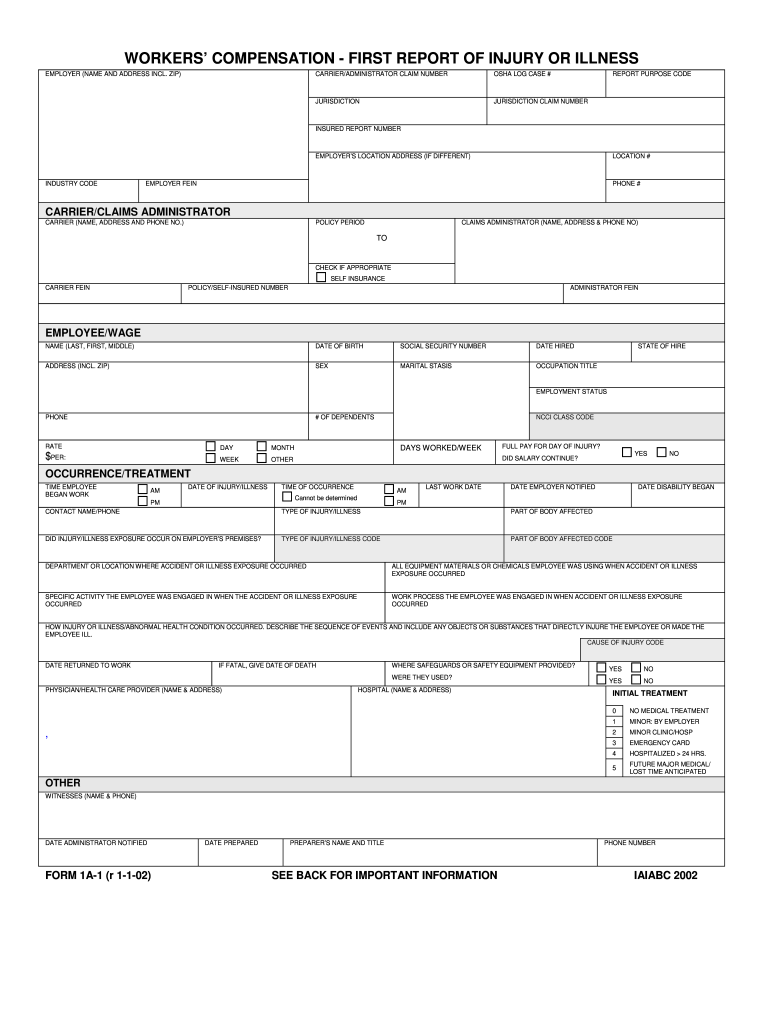
DESCRIBE THE SEQUENCE OF EVENTS AND INCLUDE ANY OBJECTS OR SUBSTANCES THAT DIRECTLY INJURE THE EMPLOYEE OR MADE THE EMPLOYEE ILL. CAUSE OF INJURY CODE DATE RETURNED TO WORK IF FATAL GIVE DATE OF DEATH WHERE SAFEGUARDS OR SAFETY EQUIPMENT PROVIDED WERE THEY USED PHYSICIAN/HEALTH CARE PROVIDER NAME ADDRESS HOSPITAL NAME ADDRESS INITIAL TREATMENT MINOR BY EMPLOYER NO MEDICAL TREATMENT MINOR CLINIC/HOSP EMERGENCY CARD HOSPITALIZED 24 HRS. FUTURE MAJOR MEDICAL/ LOST TIME ANTICIPATED WITNESSES NAME...
pdfFiller is not affiliated with any government organization
Get, Create, Make and Sign form workers compensation report form
Edit your form first report injury form form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
Share your form instantly
Email, fax, or share your form workers first report form via URL. You can also download, print, or export forms to your preferred cloud storage service.
Editing workers compensation report injury form online



Use the instructions below to start using our professional PDF editor:
1
Log in to account. Start Free Trial and sign up a profile if you don't have one.
2
Prepare a file. Use the Add New button. Then upload your file to the system from your device, importing it from internal mail, the cloud, or by adding its URL.
3
Edit form first report injury blank. Add and replace text, insert new objects, rearrange pages, add watermarks and page numbers, and more. Click Done when you are finished editing and go to the Documents tab to merge, split, lock or unlock the file.
4
Get your file. Select the name of your file in the docs list and choose your preferred exporting method. You can download it as a PDF, save it in another format, send it by email, or transfer it to the cloud.
With pdfFiller, dealing with documents is always straightforward.
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
How to fill out form workers compensation injury pdf
How to fill out MD 1A-1
01
Gather all necessary personal information including your full name, address, and contact details.
02
Obtain the MD 1A-1 form from the appropriate authority or download it from an official website.
03
Carefully read the instructions provided on the form to understand all requirements.
04
Begin filling out the form starting with your personal information in the designated fields.
05
Provide additional details as required, such as date of birth and social security number.
06
If applicable, fill out sections regarding employment information and financial details.
07
Review the completed form for accuracy to ensure all information is correct and complete.
08
Sign and date the form at the end as required.
09
Submit the form as directed, either in person, by mail, or electronically.
Who needs MD 1A-1?
01
Individuals applying for certain benefits or services that require the MD 1A-1 form.
02
Applicants needing to provide personal and financial information for verification purposes.
03
People seeking assistance from government programs or agencies that request this documentation.
Fill
first report of injury form pdf
: Try Risk Free
People Also Ask about form workers compensation injury
What does Froi mean?
Work comp: First Report of Injury (FROI) form information.
What is the report of injury form in Texas?
Form DWC-1 Employer's First Report of Injury or Occupational Disease. The employer is required to submit this form with EMPLOYERS and the injured employee or the injured employee's attorney within eight days after the employee's absence from work or notice of the Injury or Occupational Disease.
What is a first report of injury form Kentucky?
Form 1A-1 First Report of Injury (FROI). As soon as you have been notified of a work-related injury, please fill out this form and submit it to EMPLOYERS. This form must be completed within 10 days from notice of an accident. Fatalities must be reported within 24 hours.
What is the first report of injury form in Louisiana?
The First Report of Injury (Form LWC-WC IA-1) is a legal form released by the Louisiana Workforce Commission - a government authority operating within Louisiana. Louisiana Law requires that employers complete the form within 10 days of actual knowledge of the incident.
What must the first report of injury contain?
The Employer's First Report of Injury or Illness provides information on the claimant, employer, insurance carrier and medical practitioner necessary to begin the claims process. Details of the claimant's employment and circumstances surrounding the injury or illness are also requested.
What is a DWC005 form?
DWC005, Employer Notice of No Coverage or Termination of Coverage. DWC020SI, Self-Insured Governmental Entity Coverage Information. Steps to electronically submit a form to the Division of Workers' Compensation: Open the form: Google Chrome and Microsoft Edge.
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
Can I create an eSignature for the form workers injury in Gmail?
You may quickly make your eSignature using pdfFiller and then eSign your form 1a 1 right from your mailbox using pdfFiller's Gmail add-on. Please keep in mind that in order to preserve your signatures and signed papers, you must first create an account.
How do I edit first report of injury form on an iOS device?
Use the pdfFiller app for iOS to make, edit, and share form 1a 1 printable from your phone. Apple's store will have it up and running in no time. It's possible to get a free trial and choose a subscription plan that fits your needs.
How do I edit workers first report injury form on an Android device?
Yes, you can. With the pdfFiller mobile app for Android, you can edit, sign, and share 1a 1 compensation form on your mobile device from any location; only an internet connection is needed. Get the app and start to streamline your document workflow from anywhere.
What is MD 1A-1?
MD 1A-1 is a specific form used for reporting certain financial information as required by regulatory authorities.
Who is required to file MD 1A-1?
Entities that meet certain regulatory criteria, such as investment companies or businesses involved in specific financial activities, are required to file MD 1A-1.
How to fill out MD 1A-1?
To fill out MD 1A-1, you need to provide detailed information related to your financial activities, following the guidelines and sections outlined in the form.
What is the purpose of MD 1A-1?
The purpose of MD 1A-1 is to ensure transparency and accurate reporting of financial data to regulatory bodies, which aids in monitoring compliance and financial health.
What information must be reported on MD 1A-1?
MD 1A-1 requires reporting of financial statements, disclosures regarding business operations, management discussion, and any other relevant financial information.
Fill out your MD 1A-1 online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Workers Compensation First Report is not the form you're looking for?Search for another form here.
Keywords relevant to first report injury illness form
Related to form workers injury illness






If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
