MD 1A-1 2002-2024 free printable template
Show details
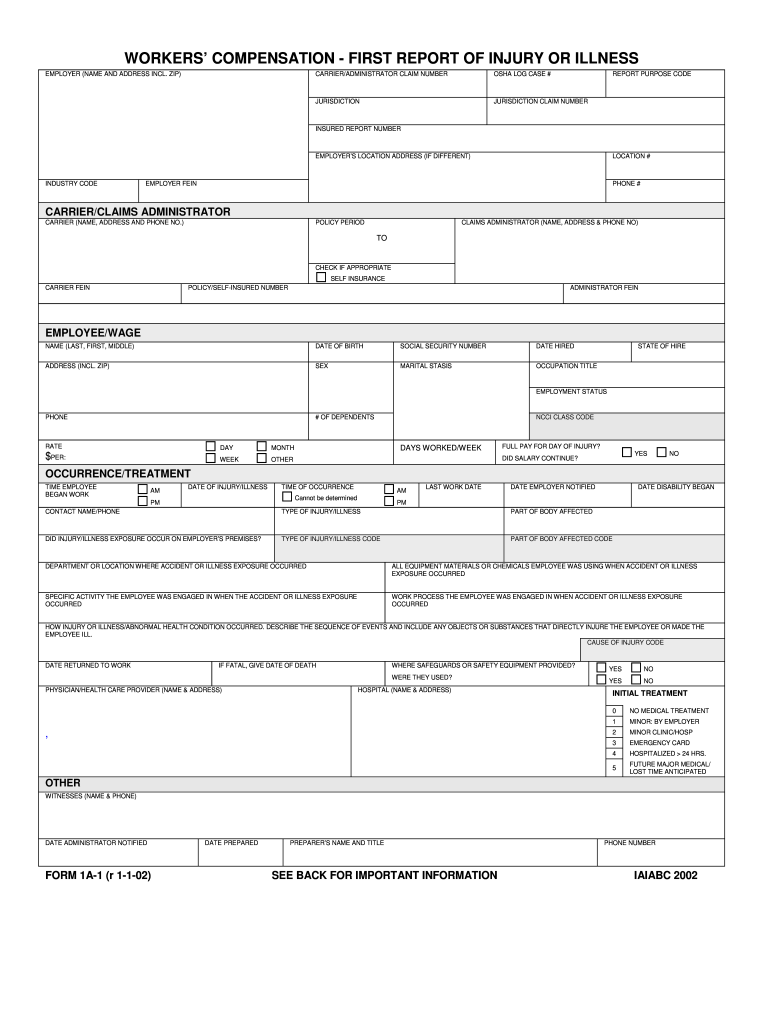
DESCRIBE THE SEQUENCE OF EVENTS AND INCLUDE ANY OBJECTS OR SUBSTANCES THAT DIRECTLY INJURE THE EMPLOYEE OR MADE THE EMPLOYEE ILL. CAUSE OF INJURY CODE DATE RETURNED TO WORK IF FATAL GIVE DATE OF DEATH WHERE SAFEGUARDS OR SAFETY EQUIPMENT PROVIDED WERE THEY USED PHYSICIAN/HEALTH CARE PROVIDER NAME ADDRESS HOSPITAL NAME ADDRESS INITIAL TREATMENT MINOR BY EMPLOYER NO MEDICAL TREATMENT MINOR CLINIC/HOSP EMERGENCY CARD HOSPITALIZED 24 HRS. FUTURE MAJOR MEDICAL/ LOST TIME ANTICIPATED WITNESSES NAME...
pdfFiller is not affiliated with any government organization
Get, Create, Make and Sign

Edit your workers compensation first report form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.

Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.

Share your form instantly
Email, fax, or share your workers compensation first report form via URL. You can also download, print, or export forms to your preferred cloud storage service.
Editing workers compensation first report online



Use the instructions below to start using our professional PDF editor:
1
Log in to account. Start Free Trial and sign up a profile if you don't have one.
2
Prepare a file. Use the Add New button. Then upload your file to the system from your device, importing it from internal mail, the cloud, or by adding its URL.
3
Edit form workers compensation injury. Add and replace text, insert new objects, rearrange pages, add watermarks and page numbers, and more. Click Done when you are finished editing and go to the Documents tab to merge, split, lock or unlock the file.
4
Get your file. Select the name of your file in the docs list and choose your preferred exporting method. You can download it as a PDF, save it in another format, send it by email, or transfer it to the cloud.
With pdfFiller, dealing with documents is always straightforward.
How to fill out workers compensation first report

How to fill out workers compensation first report:
01
Obtain the necessary forms: To fill out the workers compensation first report, you will first need to obtain the required forms from your employer or the workers compensation insurance company. These forms typically include an employee portion and an employer portion.
02
Provide personal information: Start by providing your personal information on the employee portion of the form. This typically includes your full name, address, phone number, social security number, and date of birth. Ensure that all the information provided is accurate.
03
Provide details about the injury or illness: Next, you need to describe the details of the injury or illness that occurred at work. Include information such as the date, time, and location of the incident. Explain how the injury or illness occurred and provide a clear and concise account of what happened.
04
Describe the extent of the injury: Indicate the specific body part or system affected by the injury or illness. Provide a detailed description of the symptoms and how they impact your ability to work. Include any medical treatment you have received or plan to receive related to the injury.
05
Report any witnesses: If there were any witnesses to the incident, provide their names and contact information. Witnesses can be crucial in supporting your case and verifying the occurrence of the injury or illness.
06
Sign and date the form: After completing all the necessary sections, review the information provided on the form and make sure it is accurate and complete. Sign and date the form, acknowledging that the information you have provided is true and accurate to the best of your knowledge.
Who needs workers compensation first report:
01
Employees: Any employee who sustains a work-related injury or illness needs to file a workers compensation first report. This includes full-time and part-time employees, as well as temporary and seasonal workers.
02
Employers: Employers are also required to submit the employer portion of the workers compensation first report. This allows them to report the incident from their perspective and provide any necessary information about the workplace conditions at the time of the incident.
03
Insurance companies: Workers compensation insurance providers require the first report to properly evaluate and process the claim. They rely on this report to determine the eligibility for benefits and to initiate the claims process.
Remember, the requirements for the workers compensation first report may vary based on your jurisdiction and the specific laws and regulations in place. It is important to consult with your employer or the workers compensation insurance company to ensure you are completing the report correctly and in accordance with the applicable guidelines.
Fill maryland first report injury form : Try Risk Free
People Also Ask about workers compensation first report
What does Froi mean?
What is the report of injury form in Texas?
What is a first report of injury form Kentucky?
What is the first report of injury form in Louisiana?
What must the first report of injury contain?
What is a DWC005 form?
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
What is form first report injury?
A Form First Report of Injury (FFRI) is a document used to report any work-related injury or illness that requires medical treatment beyond first aid. It is typically completed by the employee and their supervisor and submitted to the employer or workers’ compensation insurance carrier. The form includes information about the injury, including the date, time, and location of the incident, as well as details about the injury itself. It also includes information about the employee, such as their name, contact information, and Social Security number.
Who is required to file form first report injury?
The employer is required to file a First Report of Injury with their state workers' compensation agency within a certain timeframe after an employee has suffered a work-related injury or illness.
How to fill out form first report injury?
1. Gather the information you will need to complete the form. This information includes the injured worker's name, date of birth, Social Security number, address, telephone number, and date of injury.
2. Provide the employer's name, address, and telephone number.
3. Describe the injury or illness in detail, including the date, time, and circumstances of the incident.
4. Provide details of the medical treatment received, including the name, address, and telephone number of the facility or doctor.
5. Indicate whether the injured worker is able to continue working and, if not, the expected date of return to work.
6. List any witnesses to the incident and provide their contact information.
7. Sign and date the form.
8. Submit the form to the appropriate state or federal agency.
What is the purpose of form first report injury?
Form First Report of Injury (FFR) is a document used in the workplace to report an injury or illness that occurs on the job. It is a legal requirement for employers to complete this form and submit it to the relevant regulatory body within a certain timeframe. The FFR is used to ensure that injured employees receive appropriate medical treatment and benefits, as well as to ensure compliance with the relevant workplace health and safety regulations.
What is the penalty for the late filing of form first report injury?
The penalty for late filing of Form First Report of Injury (FROI) is a civil monetary penalty of up to $7,000 per violation. The penalty may be assessed to the employer, the insurer, the third party administrator, or the self-insured.
What information must be reported on form first report injury?
The specific information required on a first report of injury form may vary depending on the jurisdiction and the company's internal policies. However, some common information that is typically included on such forms may include:
1. Employee information: Name, address, contact details, job title, department, and other relevant identification information of the injured employee.
2. Employer information: Name, address, contact details, and any other relevant identification information of the employer or company.
3. Date and time of the injury: The specific date and time at which the injury occurred or was first reported.
4. Location of the injury: The specific place or location where the incident occurred.
5. Description of the incident: A detailed account of how the injury occurred, including any contributing factors or events leading up to the incident.
6. Type and extent of injury: The nature and severity of the injury sustained, including specific details such as body parts affected, medical diagnosis, and extent of medical treatment required.
7. Witnesses: Any witnesses to the incident and their contact information.
8. Supervisor's report: Details of the supervisor or manager present at the time of the incident, including their observations and actions taken.
9. Reporting time frame: Whether the injury was reported within the required time frame or if there was any delay in reporting.
10. Other relevant information: Any other pertinent details related to the incident or injury, such as prior medical conditions, safety precautions in place at the time, or potential third-party liability.
It is important to consult with local laws and regulations or company policies to ensure that all required information is included on the first report of injury form.
Can I create an eSignature for the workers compensation first report in Gmail?
You may quickly make your eSignature using pdfFiller and then eSign your form workers compensation injury right from your mailbox using pdfFiller's Gmail add-on. Please keep in mind that in order to preserve your signatures and signed papers, you must first create an account.
How do I edit form workers compensation report on an iOS device?
Use the pdfFiller app for iOS to make, edit, and share form first report injury form from your phone. Apple's store will have it up and running in no time. It's possible to get a free trial and choose a subscription plan that fits your needs.
How do I edit workers compensation first report form on an Android device?
Yes, you can. With the pdfFiller mobile app for Android, you can edit, sign, and share form first report injury on your mobile device from any location; only an internet connection is needed. Get the app and start to streamline your document workflow from anywhere.
Fill out your workers compensation first report online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Form Workers Compensation Report is not the form you're looking for?Search for another form here.
Keywords relevant to form 1a 1 form
Related to workers compensation report injury







If you believe that this page should be taken down, please follow our DMCA take down process
here
.
